CASE NOTES
Unilateral pyothorax in an Angus heifer
Bruce Watt, Central Tablelands Local Land Services, Bathurst, Bernadette O'Brien, final year veterinary student at Charles Sturt University and Erika Bunker, Elizabeth Macarthur Agricultural Institute, Menangle
Posted Flock and Herd November 2023
Introduction
Unilateral pyothorax is a rare finding in cattle. Causes include traumatic reticuloperitonitis, a ruptured pulmonary or mediastinal abscess (including mediastinal abscessation following haematogenous spread of septic microemboli from a liver abscess) (McLennan & McGowan, 1995), lymphatic spread from a septic abdominal process (Parkinson et al. 2019) and following aspiration pneumonia (from either faulty administration of an oral drench or inhalation of ruminal contents) (Scott, 2012; Panciera & Confer, 2010).
In this case in an Angus heifer, the cause was not determined although traumatic reticuloperitonitis was ruled out.
History
On Thursday 27 April 2023, a 20-month-old Angus heifer was examined after a Central Tablelands producer reported that the heifer had been lethargic with a swollen brisket for several weeks. The heifer had been weaned in March 2022 and had been running on a mix of native and improved pasture. She had not received any recent treatment and was due to calve in June, 2023. The producer had noticed that the heifer had been lethargic on mustering to the yards. She also had noticeable weight loss and diarrhoea.
Clinical findings
On physical examination, the heifer had a poor body condition score (2/5) and a rough coat. She was quiet, but alert and responsive. Marked pitting oedema was evident under the mandible, brisket, and abdomen (Image 1). The heifer was tachycardic (112 beats per minute), tachypnoeic (44 breathes per minute) and pyrexic (39.6°C). On thoracic auscultation, faint heart sounds as well as rales on inspiration and expiration could be heard on the left, but neither lung nor heart sounds were detected on the right. The heifer stood with abducted elbows. The heifer also had mild bilateral clear mucoid nasal discharge and pale pink vulval mucous membranes.
Laboratory findings
Bloods were submitted to the laboratory. Haematology revealed a stress leukogram, with a moderate neutrophilia and lymphopaenia. Biochemistry revealed a mild hyperglobulinaemia and a mild hypoalbuminaemia. There was moderately elevated BHB and hypoglycaemia. There was hypercreatinemia, a moderate elevation in GLDH and GGT and mild hyperphosphataemia and hypochloraemia. Glutathione peroxidase (GSHPx) was mildly elevated.
The heifer was also tested for pestivirus, liver fluke, and enzootic bovine leucosis. All results were negative.
NECROPSY FINDINGS
On Monday 8 May 2023, as the heifer was deteriorating, she was euthanised and necropsied. The heifer was in poor condition (BCS 1.5/5). There was no gross evidence of actinobacillosis on palpation of the tongue. There was marked generalised ventral oedema from mandible to ventral abdomen. The oedema was clear to straw coloured and 5-10cm thick (Image 2).
Within the right thoracic cavity, there was approximately 10L of yellow turbid foul-smelling fluid (Image 3) and a large yellow fibrinous clot (approximately 1kg). The pleural surface of the right thoracic cavity was covered in 2cm of thick yellow material (Image 4). The right lung was small and collapsed (Image 5). The left lung and pleura were relatively normal (Image 6). The heart was soft and globoid, with the right side appearing relatively enlarged (Image 7).
Within the abdominal cavity, there was approximately 10L of clear yellowy-brown fluid. The liver was mildly enlarged, with rounded edges. On the cut liver, there were large irregular patches of light brown tissue with smaller patches of adjoining dark red tissue (Image 8). Within the abomasum, there were several 5mm mucosal ulcers. There were focal 3cm oval dark purple areas visible on the serosal surface of the small intestines. The kidneys appeared grossly normal and there was a foetus within the right uterine horn at five months gestation.

Image 1. Affected heifer showing marked ventral oedema

Image 2. Initial opening of the peritoneal cavity showing marked ventral oedema and ascites

Image 3. Right thoracic cavity showing pyothorax

Image 4. Right thoracic wall showing extensive, chronic pleurisy

Image 5. Collapsed right lung

Image 6. Unaffected left thoracic wall

Image 7. Heart

Image 8. Liver cut section
LABORATORY FINDINGS
Samples of the left and right lung left, right ventricles, liver, small intestine and kidneys were submitted for histological examination. The thick yellow material on the right pleural surface was submitted for culture and testing. Exclusion testing for contagious bovine pleuropneumonia (CBPP) was requested.
Bibersteinia trehalosi was cultured while Mycoplasma spp were not isolated.
Histopathology revealed severe and chronic liver lesions suggestive of an ongoing hypoxic insult, consistent with heart failure (Image 9). The lesions were severe enough to cause liver failure, which could have contributed to oedema and effusions. There were no histological lesions suggestive of a cardiomyopathy as a cause of heart failure, however an anatomical or functional deficit was another possibility. In this case heart function may have been compromised by the extensive pleural effusion, which would also have caused respiratory difficulties and hypoxic damage to the liver.
The microscopic lung changes were unusual, with mucus but not purulent exudate filling alveoli and bronchioli, with relatively sparse inflammatory cells (Image 10). Other less significant histological lesions included a focal acute erosive and haemorrhagic abomasal lesion, most likely a secondary complication, and a mild chronic lymphocytic interstitial nephritis, a common incidental finding. There were no necro-suppurative lesions typical for B. trehalosi infection/septicaemia in lung or liver parenchyma, which indicates that the infection was mostly confined to the parietal pleura, with only a mild fibrinous exudate seen on the serosal surface of lung and liver.
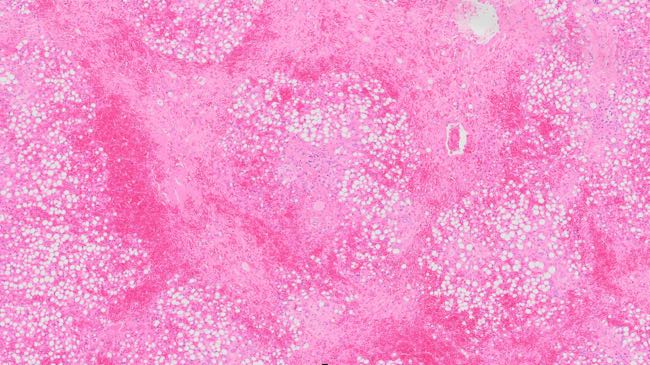
Image 9. Liver, pattern of severe periacinar hepatocyte loss with replacement by fibroplasia and haemorrhage, and severe fatty degeneration of remaining hepatocytes. H&E stain, 5x.
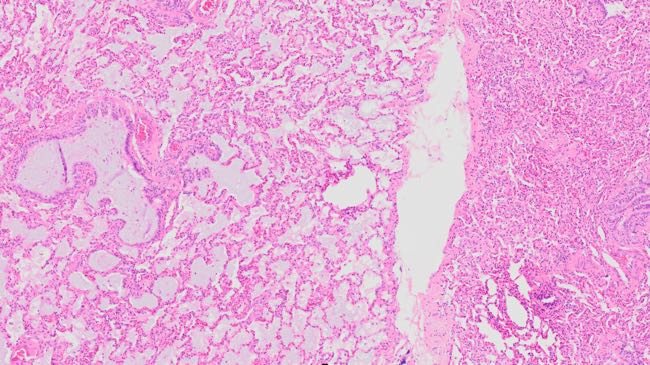
Image 10. Lung, lobular pattern of mucus filled alveoli and bronchiole (lobule on left side of image) and atelectasis (lobule on right side of image). H&E stain, 5x.
Discussion
Marked antero-ventral oedema is occasionally seen on the Central Tablelands in cattle with traumatic reticuloperitonitis, cardiomyopathy, thymic lymphoma and chronic liver disease. The authors have not seen pyothorax in a cow previously.
In this case, there was no evidence of a penetrating foreign body between the reticulum and the thoracic cavity. Scott (2012) commented that pyothorax associated with traumatic reticuloperitonitis typically affect the left side of the thorax. There was evidence of both a pleuritis and hepatopathy. Based on the necropsy and histopathology findings, the most likely cause of the unilateral pyothorax was hypothesised to be a ruptured abscess in the right thorax.
The most likely cause of peripheral oedema in this heifer was the right unilateral pyothorax impeding cardiac function. The pyothorax would have resulted in right-sided heart failure and hepatopathy, which led to the subcutaneous oedema and ascites found on clinical examination and necropsy.
Samples were tested for Mycoplasma including M. mycoides subsp. mycoides, the cause of CBPP, although the lung lesions were not suggestive of a Mycoplasma infection. CBPP is now exotic to Australia, with the last case seen in 1967 and freedom declared in 1973 (Parkinson et al. 2019, World Organisation for Animal Health, 2023). CBPP causes a fibrinous pleuropneumonia that may be unilateral and is characterised by a copious often yellow pleural effusion (Di Teodoro, 2020; Chase et al. 2017). Laboratory testing was therefore requested with CBPP excluded.
Acknowledgements
The authors would like to thank the producer for his cooperation in investigating this case.
References
- Chase C, Lutz K, McKenzie E & Tibary A (Eds.) (2017) Blackwell's five-minute veterinary consult: Ruminant John Wiley & Sons, Incorporated
- Di Teodoro G, Marruchella G, Di Provvido A, D'Angelo AR, Orsini G, Di Guiseppe P, Sacchino F & Scacchia M (2020) Contagious bovine pleuropneumonia: A comprehensive overview Veterinary Pathology 57(4):476-489 doi.org
- Eclinpath (2020) Glucose eclinopath.com
- Keleş I, Alptekin I, Atasoy N, Çinar A, Dönmez N & Ceylan E (2003) Pseudopericarditis in a cow caused by theileriosis - A case report Veterinarski Arhiv 73(2):111-117
- McLennan M & McGowan M (1995) Pyothorax in a Friesian bull Australian Veterinary Journal 72(3):115-116 doi.org
- Panciera RJ & Confer AW (2010) Pathogenesis and pathology of bovine pneumonia The Veterinary Clinics of North America Food Animal Practice 26(2):191-214 doi.org
- Parkinson TJ, Vermunt JJ, Malmo J & Laven R (Eds.) (2019) Diseases of cattle in Australasia Massy University Press
- Scott P (2012) Inhalation pneumonia (aspiration pneumonia) in adult cattle UK-Vet Livestock 17(7):17-19 doi.org
- World Organisation for Animal Health (2023) Contagious bovine pleuropneumonia www.woah.org