FOOT AND MOUTH DISEASE: A DIAGNOSTIC CHALLENGE
Steve Eastwood, District Veterinarian, Northern Tablelands LLS, Armidale
Posted Flock & Herd March 2015
Foot-and-mouth Disease (FMD) is often described in context of the typical clinical presentation in pigs and cattle. What is less recognised is that presentation in sheep can be varied and often difficult to diagnose in the field. The movement of infected, clinically normal sheep through the saleyard system of the UK caused the spread of FMD throughout the UK in 2001. Australian veterinarians need to avoid focussing solely on ‘textbook’ outbreaks as misdiagnosis may be the difference between a $6 billion regional response and a $52 billion multistate response (ABARES, 2013).
FMD EXPRESSION
FMD virus typically presents in cloven hoofed animals with fever, lameness and vesicular lesions on snout, mouth, feet and teats. In young animals, it may also cause death due to myocarditis without vesicular lesions.
The lesions and clinical signs will vary due to a wide range of host, agent and environment factors including the strain/serotype of the virus, the species involved and immunity of the herd/flock (Mansley, 2004).

Figure 1: FMD in cattle (UK 2001)

Figure 2: FMD in pigs (Nepal, 2013)

Figure 3: FMD in sheep - dental pad 3 day old lesion (Sourced from DEFRA website)

Figure 4 FMD in sheep - blanching of the coronary band (2 day old lesions)
FMD STRAIN/SEROTYPE
The FMD virus is classified by serotype and strain. There are seven serotypes A, O, Asia 1, SAT 1, SAT 2, SAT 3 and C (See Figure 3 for distribution). Within each serotype are topotypes (which demonstrate at least 15% genetic variability) and within each topotype there are multiple strains. Immunity is serotype specific.
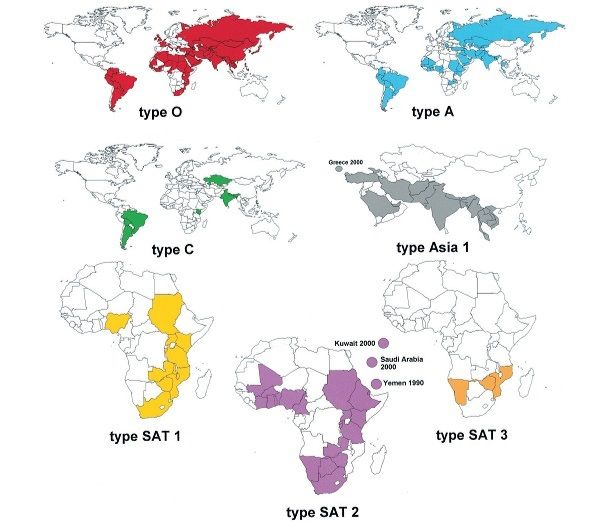
Figure 5: Countries in which FMD was reported to the OIE between 1990 and 2002. The data and maps were compiled by Nick Knowles and can be found at www.iah.bbsrc.ac.uk/virus/picornaviridae/apthovirus
Serotype O was isolated from >60% of the positive FMD samples received at the World Reference Laboratory at Pirbright, UK between 2000 and 2005 (Knowles, 2005).
Strains express differently in different species. For example the Cathay strain type O virus is mainly confined to pigs (Windsor, 2011). However there are other strains of serotype O that are well adapted to small ruminants.
PanAsia Serotype O virus is a pandemic strain which emerged in the 1990's from Southern Asia as a new strain and spread to Korea, Japan, Russia, Mongolia, South Africa, the United Kingdom, Republic of Ireland, France, and the Netherlands between 1998 and 2001 (Knowles, 2005). It presents in typical textbook fashion in both pigs and cattle however clinical signs in sheep are mild (Watson, 2004).
SPECIES DIFFERENCES
According to Hughes et al. (2002) "Cattle and pigs develop obvious signs of FMD". However, the UK outbreak in 2001 demonstrated how difficult it is to make a clinical diagnosis of FMD in sheep. Where samples were submitted, over 50% of flocks slaughtered were not confirmed positive for FMD. Being difficult to diagnose meant that disease was spread to other livestock prior to detection and as a result sheep played a major role in the outbreak (Kitching, 2002).
Sheep are highly susceptible to FMD virus infection via aerosol and can excrete airborne virus; however, during outbreaks they are most likely infected by contact with infected animals. Sheep to sheep spread is restricted with silent transmission more likely before clinical signs are observed (Kitching, 2002; Hughes et al. 2002). This demonstrates variable intra-flock infection rates and is supported by data from one farm where there were 91% cattle clinically affected compared with only 5% sheep seropositive (Kitching, 2002).
FLOCK IMMUNITY
Sheep are known to carry the virus for up to 9 months (Mansley, 2004). These carrier sheep have the potential to become a source of infection for other properties. In flocks where FMD is endemic it may only be clinically detectable in naive animalse.g. lambs or newly introduced stock.
Discussion
The textbook FMD scenario of slobbering, lame cattle or depressed, lame pigs equates to FMD vesicular lesions in mouth, feet and udder. This is unlikely to be seen in sheep. Clinical disease in sheep is characterized by lesions on the feet and mouth, with fever and viraemia. However Hughes et al. (2002) reported that up to 25% of infected sheep may fail to develop lesions, and an additional 20% may form only one lesion, with the mean time for lesion recognition being only 2.2 days and 93% of lesions occurring in the feet.
The presence of mouth lesions in sheep had gone relatively unreported in the UK until the FMD outbreak in 2001 when veterinarians began examining sheep mouths in more detail. The difficulty in making a clinical diagnosis in sheep during the UK outbreak was compounded by the presence of oral lesions due to "OMAGOD" (Ovine Mouth and Gum Obscure Disease) or "Idiopathic oral ulcers" (Figure 6). The majority of these types of oral lesions are due to trauma and are found at the lower gum below the incisors. However lesions were also found on the dental pad and these caused significant concern for veterinarians during the UK outbreak and many flocks were slaughtered as a result of misdiagnosis (Watson, 2004). In Australia oral lesions in sheep do occur and are often associated with trauma due to hard ground, harsh feed and thistles. Veterinarians should regularly check mouths when examining sheep to become familiar with the normal presentation of these lesions.

Figure 6: Idiopathic oral ulcers - Credit Phil Watson VLA Penrith (Sourced from DEFRA website)
In a DEFRA (2003) commissioned study in 2001 over 20,000 sheep heads were examined for oral lesions due to idiopathic oral ulcers. Approximately 1% of all sheep examined had oral lesions meeting the criteria (Reference).
Also in this study, 38 veterinarians with experience in FMD diagnosis were tested on their ability to diagnose FMD based on photographs of lesions in sheep. The range of correct diagnoses ranged from 53% to 93% and the mean was 74%. Making a diagnosis from photographs ignores the fact that a clinical examination plus collection of history would generally have taken place. However it identifies the variability in veterinarians’ approaches and all participants had recent experience with diagnosing FMD on farm. In addition participants knew they had to have FMD as a differential diagnosis as they were asked to exclude/diagnose FMD. Contrast this with Australian conditions where veterinarians and stock inspectors may be called out to a farm for a routine diagnostic visit due to the odd lame sheep, with little FMD diagnostic experience and other endemic diseases at the forefront of their minds.
In the same study, information about lesions found on infected farms was compared with confirmed laboratory results. The presence of dental pad lesions (of any size) gave a high sensitivity (90.5%) and specificity (84.3%). The specificity was increased by combining the dental pad lesions with coronary band or interdigital lesions, with a reduction in sensitivity.
Conclusion
Diagnosing FMD in sheep is difficult. Veterinarians who investigate disease outbreaks involving lameness in sheep, the most common clinical sign in FMD, should undertake a thorough clinical examination and maintain FMD as a possible differential diagnosis. Where appropriate, laboratory samples should be submitted for exclusion.
References
- ABARES (2013) Research Report. apo.org.au
- DEFRA (2003) Final Project Report. sciencesearch.defra.gov.uk: Analysis of lesion profiles in sheep with foot and mouth disease and idiopathic mouth ulcers
- Hughes GJ, Mioulet V, Kitching RP, Woolhouse MEJ, Alexandersen S, Donaldson AI. Foot and mouth disease virus infection of sheep: implications for diagnosis and control. The Veterinary Record 2002;150:724-727
- Kitching RP, Hughes GJ. Clinical variation in foot and mouth disease: sheep and goats. Rev Sci Tech Off Int Epiz 2002;21(3):505-512
- Knowles, N.J., Samuel, A.R., Davies, P.R., Midgley, R.J., and Valarcher, J. Pandemic Strain of Foot-and-Mouth Disease Virus Serotype O. Emerging Infectious Diseases. 2005;11(12);1887-1893
- Mansley LM. The challenge of FMD control in the 2001 UK FMD epidemic. International Society for Animal Hygiene 2004;345-350
- Watson P. Differential diagnosis of oral lesions and FMD in sheep. In Practice 2004;26:182-191
- Windsor PA, Freeman, PG, Abila R, Benigno C, Verin B, Nim V, Cameron, A. Foot-and-Mouth Disease Control and Eradication in the Bicol Surveillance Buffer Zone of the Philippines. Transboundary and Emerging diseases. 2011;58:421-433