CASE NOTES
Foot and mouth disease in Kenya
Paul Freeman, Regional Veterinary Officer, NSW Department of Primary Industries
Posted Flock & Herd March 2012
Overview of key features
Foot-and-mouth Disease (FMD) is a highly contagious disease of cloven footed animals. It is economically significant affecting both production and trade access. The disease is caused by a small non enveloped RNA virus with 7 immunologically distinct serotypes.
Distribution

Susceptible species
Natural: ruminants and pigs mainly but over 70 species are susceptible (e.g. African buffalo, deer, antelope, warthog, wild boar).
Experimental: elephants, some small rodents can be infected but little role in the epidemiology of the disease.
Incubation period: 2-14 days but can be as short as 24 hrs. The duration of the incubation period is strongly related to dose.
Route of infection
Inhalation - main route for ruminants. Pigs need 600 x dose for this route
Ingestion - higher doses needed compared to via inhalation route but is the main route for pigs
Through damaged skin or mucosa - grass seeds, rough feedstuffs, teat lesions, footrot.
Excretion of virus
Virus is excreted in all body discharges (urine, saliva, milk, faeces, semen) and in expired air. The concentration of virus in expired air from infected pigs is 3000 times greater than the level in expired air from infected castle. The duration of excretion can start 4 days before clinical signs and usually ceases 4-5 days after vesicles develop.
Environmental survival
The virus can survive up to 6 mths in favourable cool conditions. It does not like hot dry conditions. In human nasal cavity it can persist for up to 48 hours.
Immunity
Antibodies first appear 3-5 days after onset of clinical signs. They remain elevated for a long time in ruminants (years) but only months in pigs. While antibodies clear virus from most sites virus can persist in the oropharynx and lead to development of a carrier state in ruminants but not in pigs. In ruminants the carrier state can persist for years ( buffalo 5 yrs, cattle 3.5 yrs, sheep 9 months, goats 4 months). In the carrier state virus shedding is low level and intermittent and there is a lack of consensus about the significance of the carrier state in FMD epidemiology.
Diagnosis
While the clinical picture in acute outbreaks with multiple animal involvement is fairly typical, chronic infection can be confused with a range of other diseases such as bluetongue, other vesicular diseases, cowpox, infectious bovine rhinotracheitis, malignant catarrhal fever, peste des petits ruminants, bovine viral diarrhoea virus, scabby mouth as well as other physical and toxic insults.
Laboratory testing

Lateral Flow device (LFD)
This is a new pen side test that has been used in FMD field outbreaks. It uses epithelium or vesicular fluid and gives a result in minutes.
ELISA to detect antibodies to non structural proteins (NSP)
Infection induces antibodies against the non structural proteins involved in virus replication whereas vaccination does not normally and ELISA tests are available to distinguish vaccination titres from infection titres. This distinction is not as clear cut when multiple vaccinations have been undertaken.
Vaccination
All vaccines are killed and do not provide cross protection against other serological strains so multi-valent vaccines are required as several strains may be active at the same time. Vaccination only offers short term immunity and vaccinated animals can be sub clinically infected.

SAT1 is the dominant serotype in Kenya at present and reports of over
50% mortality rates were recorded on some farms.
Government veterinary services in Kenya

Estimated livestock numbers in Kenya (underestimates)

FMD control in Kenya
Up until 1986 vaccination was free for cattle and about 80% coverage achieved. Small ruminants were not vaccinated. The government then introduced costs recovery and coverage rates dropped to around 10% and remain low due to the cost of the vaccine which contains O, A, SAT1 and SAT2 serotypes.
Action following confirmation of FMD detection
A general quarantine is proclaimed and the markets are closed and sales of animals and animal products are prohibited. Ring vaccination is undertaken by government officers around outbreaks. However restricting animal movements is difficult to monitor and communal grazing often leads to local spread. Furthermore Masai herdsmen move their herds and flocks over large areas grazing traditional lands and these herds often spread FMD infection as few farms have secure boundary fencing.
EU FMD workshop in Nnakuru November 2011
The EU FMD commission hosted a 4 day workshop on FMD attended by veterinarians from mainly Europe but also 2 from Australia. We got the opportunity to examine clinical FMD cases, age lesions, collect samples for confirmation and undertake epidemiological investigations on the property to determine the source of infection and provide advice on biosecurity measures to assist the stock managers and owners with FMD control. Appropriate PPE was used during the property visits to ensure the team did not act as vectors for infection (See Figure1).

Figure 1 - PPE worn for property visits

Figure 2 - Photos of various FMD lesions and collection of probang samples.
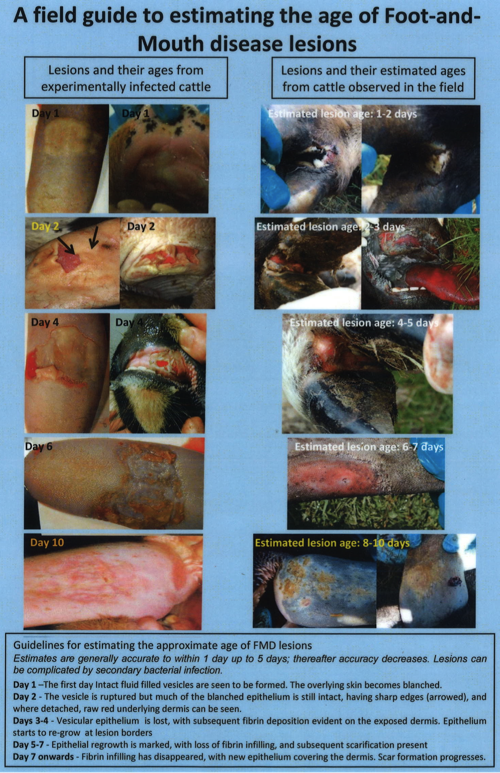

Appendix 2: Ageing FMD lesions
References
- European Commission for the Control of Foot-and-Mouth Disease. www.fao.org
- European Union FMD Training Course Handbook 2011. European Commission for the Control of Foot-and-Mouth Disease. www.fao.org