CASE NOTES
Monensin toxicity in sheep grazing a travelling stock reserve
Amy Masters, Central Tablelands Local Land Services, Orange and Mark Hazelton, NSW Animal and Plant Health Laboratories, Menangle
Posted Flock and Herd August 2023
Introduction
Monensin is a polycyclic antibiotic and ionophore produced by Streptomyces cinnamonensis1,2,3. It serves as a feed additive to control coccidiosis in several animal species and is used to promote growth and prevent bloat in ruminants4,5. Susceptibility to the toxic effects of ionophores is highly species specific with horses identified as acutely sensitive. Toxicoses occur due to accidental access to medicated feed, errors in mixing and deliberate feeding of a ration formulated for a less sensitive species4. Monensin poisoning causes degeneration and necrosis in myocardial and skeletal muscle cells5,6,7. There is no antidote or approved treatment regimen2.
This report describes a case of monensin toxicity in sheep grazing a travelling stock reserve.
Case report
History
A producer in the Molong area of NSW moved a mob of 66 sheep onto a travelling stock reserve (TSR) adjacent to his property for grazing in early May 2018. This producer had leased the TSR for more than 10 years and had never recorded any stock losses whilst grazing the area.
The mob was comprised of predominantly mature first-cross ewes at the point of lambing and a small number of older lambs from the previous season.
When the gate to the TSR was opened, the producer noticed the sheep immediately rush to a bare patch of ground and begin licking the ground. He did not investigate the area at that time.
The next morning (Day 1), six sheep were found dead, including ewes and older lambs. The producer suspected Phalaris sudden death syndrome and moved the remainder of the mob off the TSR that afternoon. All other stock appeared healthy when returned to their previous paddock.
Five additional animals were found dead on Day 4. Another seven sheep died on Day 5. The producer contacted the Central Tablelands Local Land Services (CTLLS) to investigate the unexplained deaths.
The significant findings from property visits conducted on Days 4 and 5 are summarised below.
Paddock walk
The TSR was Phalaris dominant and water was sourced from a small creek. The producer reported the reserve had not been grazed for seven months. The TSR had not received any significant recent rainfall. No toxic plants were observed. There was no known history of anthrax occurring on the reserve. There was evidence of recent tree removal near the overhead powerlines by the electricity company. The bare patch of ground licked by the sheep upon introduction to the TSR was examined and many fine (~1-2mm diameter) yellow granules were observed over a 1-1.5m diameter area (Image 1). Granules were collected for analysis.

Image 1. Fine yellow granules on bare ground
Clinical Examination
Only one sick animal (ram lamb) was available for clinical examination during the investigation as affected sheep progressed rapidly from apparently healthy, and indistinguishable from others in the mob, to dead. The ram lamb was dull, tachypnoeic and tachycardic. The rumen was inactive, and a foul-smelling scour was present. Body temperature was 37.9°C. This ram died approximately 10 minutes after clinical examination and was then necropsied.
Post-mortem examination
Anthrax was excluded by a negative immunochromatographic test (ICT). Six sheep (including ewes and older lambs) were necropsied over the course of two property visits. Animals were found to be in good body condition and in some cases, faecal staining was present on the perineum. Pulmonary oedema and mild to moderate pericardial and pleural effusions were noted. Marked abdominal effusions were observed in cases necropsied later in the disease investigation (Image 2). Mild renomegaly and hepatomegaly were present. The small intestinal contents appeared haemorrhagic and had a foul odour in some cases. Fine yellow granules consistent with those observed on the bare ground of the TSR were found in the forestomach of all sheep (Images 3, 4 and 5).

Image 2. Marked abdominal effusion

Image 3. Fine yellow granules in rumen

Image 4. Fine yellow granules in abomasum

Image 5. Fine yellow granules in abomasum
Laboratory Results
The most significant serum biochemistry changes (Table 1) in the ram lamb included marked elevations in CK and AST, suggestive of muscle damage (primary and/or secondary myopathy); moderate elevations in urea and creatinine indicative of pre-renal, renal or post-renal azotaemia, with post-renal azotaemia excluded at post-mortem; a marked hyperphosphataemia (most likely due to severe skeletal myopathy as opposed to artifact, dehydration, or renal disease); and a moderate hyperkalaemia (artifact, dehydration or renal disease). Other changes included a mild elevation in GLDH (hepatocellular damage); a moderate hyperglycaemia (likely stress-induced); a moderate hypoglobulinaemia; a mild to moderate hypocalcaemia; a mild hypermagnesaemia; and a mild elevation in Beta-Hydroxybutyrate (BHB) (ketosis).
Mild to marked elevations of urea in the aqueous humour biochemistry of all animals were consistent with the pre-renal or renal azotaemia (Table 2) identified in the ram lamb. On urinalysis of the ram lamb (Table 3), the urine was acidic and yellow brown with possible haematuria, haemoglobinuria, or myoglobinuria. The proteinuria was likely due to the haematuria, haemoglobinuria, or myoglobinuria. Myoglobinuria was considered most likely considering the other case findings.
Table 1. Ram lamb serum biochemistry results
| MBA JH Bov/Ov/Cap | |||
|---|---|---|---|
| CK | + | 21195 | < 330 U/L |
| AST | + | 4370 | (60-280) U/L |
| Bilirubin - Total | 3.0 | (1.71-8.55) umol/L | |
| GLDH | + | 27.30 | < 20 U/L |
| Creatinine | + | 237 | (106-168) umol/L |
| Urea | + | 20.6 | (2.9-7.1) mmol/L |
| Serum Protein | - | 55 | (60-79) g/L |
| Albumin | 29 | (24-30) g/L | |
| Globulin | - | 26 | (35-57) g/L |
| A:G Ratio | + | 1.12 | (0.42 -0.76) |
| Glucose | + | 8.69 | (2.8-4.4) mmol/L |
| Calcium (Uncorr.) | - | 2.22 | (2.88 3.20) mmol/L |
| Phosphate | + | 4.25 | (1.62 2.36) mmol/L |
| Magnesium | + | 1.39 | (0.90-1.26) mmol/L |
| Sodium | 143 | (139-152) mmol/L | |
| Potassium | + | 7.2 | (3.9 5.4) mmol/L |
| Chloride | 103 | (95-108) mmol/L | |
| Serum/Plasma Appearance | ++ | Haemolysis - Moderate | |
| Gamma GT | 26 | (20-52) U/L | |
| Beta-Hydroxybutyrate | + | 0.76 | (0.51-0.59) mmol/L |
Table 2. Aqueous humour biochemistry results
| SAMPLE | 07167.1.AH | 07167.2.AH | 07167.3.AH | 07167.4.AH | 07167.5.AH | |
|---|---|---|---|---|---|---|
| UREA | 2.9-7.1 mmol/L | 13.3 H | 8.1 H | 7.9 H | 8.1 H | 9.5 H |
| GLUCOSE | < 4.4 mmol/L | 0.7 | 0.2 | 0.1 | 0.0 | 0.0 |
| BHB | 0.00-0.80 mmol/L | 0.68 | 0.22 | 0.59 | 0.55 | 1.27 H |
| AQ.HU CA | 1.13-2.03 mmol/L | 1.52 | 1.73 | 1.47 | 1.50 | 1.66 |
| AQ.HU MG | 0.65-1.55 mmol/L | 0.89 | 0.96 | 0.94 | 1.04 | 1.08 |
| NITRATE | < 10 mg/L | < 10 | < 10 | < 10 | < 10 | < 10 |
| NITRITE | < 1 mg/L | < 1 | < 1 | < 1 | < 1 | < 1 |
| PHOS | 1.13-2.58 mmol/L | 1.13 | 1.27 | 1.18 | 2.29 | 1.74 |
| AMMONIA | 0-200 umol/L | 37 | 159 | 303 H | 489 H | 197 |
| D-LACT | 0.0-0.5 mmol/L | 0.0 | 0.0 | 0.1 | 0.0 | 0.0 |
Table 3. Ram lamb urinalysis results
| SAMPLE | 07305.AH.15 | 07305.AH.16 | |
|---|---|---|---|
| UREA | 2.9-7.1 mmol/L | 12.8 H | 44.7 H |
| GLUCOSE | < 4.4 mmol/L | 0.5 | 0.1 |
| BHB | 0.00-0.80 mmol/L | 0.61 | 0.42 |
| AQ.HU CA | 1.13-2.03 mmol/L | 1.55 | 1.33 |
| AQ.HU MG | 0.65-1.55 mmol/L | 1.10 | 1.23 |
| NITRATE | < 10 mg/L | < 10 | < 10 |
| NITRITE | < 1 mg/L | < 1 | < 1 |
| D-LACT | 0.0-0.5 mmol/L | 0.0 | 0.1 |
| AMMONIA | 0-200 umol/L | 292 H | 832 H |
| PHOS | 1.13-2.58 mmol/L | 1.64 | 3.00 H |
Heart histology (Image 6) of the ram lamb indicated marked, acute, multifocal to coalescing, monophasic myonecrosis with acute, diffuse myocardial degeneration and early repair. This change varied in severity with milder changes occurring in ewes that died earlier in the investigation, and more dramatic cardiac lesions with early repair in animals that took several days to die. Histologic changes of the liver and kidney of all animals examined were also present. Glomerular shrinkage with severe protein loss and tubular degeneration (Image 7) was observed in the kidneys. Liver sections revealed acute, diffuse, mild-to-moderate hepatic degeneration. Moderate, acute, multifocal pulmonary oedema was present in one ewe. Changes visible in the kidney, liver, and lung were attributed to hypoxic damage associated with circulatory failure due to the cardiac disease. Myoglobinaemia may have contributed to the renal lesions.

Image 6. Ram lamb, heart: myonecrosis, monophasic, acute, multifocal, marked with marked myocardial degeneration and early repair. Cardiomyocytes were often ruptured, with contraction and were associated with mild infiltration of macrophages and proliferation of fibroblasts.
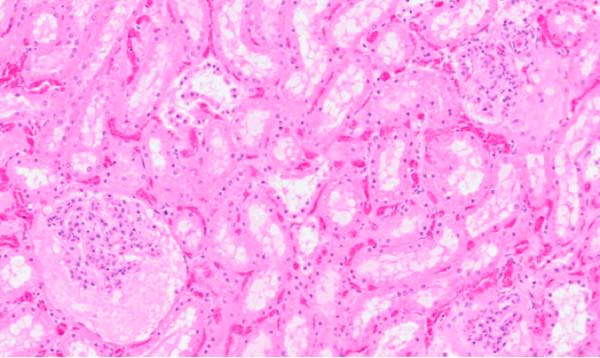
Image 7. Ram lamb, kidney: Glomerular shrinkage and expansion of Bowmans capsule by proteinaceous fluid (protein loss) and tubular degeneration.
Toxicological analysis
A sample of the yellow granules collected from the TSR was submitted to the Chemical Residues Laboratory in Queensland. Analysis confirmed the substance contained 0.5g/kg monensin.
Outcome
Laboratory confirmation that the yellow granules contained monensin prompted an investigation into the most likely source of the substance and prompted the producer to divulge that he had allowed another farmer to graze Merino wethers on the TSR in February 2018. The owner of the wethers reported feeding a mineral concentrate premix directly in a trough (without incorporating the product into feed as instructed on the label). No wethers became ill or died. Upon removing the wethers from the reserve, the remaining product was tipped onto the ground where it was later discovered by the sheep introduced in May. When compared to the original premix, it would appear the salt/mineral component had dissolved, possibly due to weathering or rain exposure, leaving behind the insoluble monensin granules. Perhaps traces of palatable salt resided in the contaminated soil, enticing the sheep to lick the bare ground. Ionophores are not typically palatable. The salt content may have also limited consumption of the original product and could explain why the wethers suffered no ill effects despite consuming the product directly without it being mixed with feed.
Interestingly, the product the farmer reportedly fed the wethers (Olsson's Sheep Mix®) contains the ionophore lasalocid not monensin. In an attempt to verify the ionophore listed on the labelled ingredients, an unopened bag of the sheep product was examined from the same pallet of mix in the farmer's shed that had been fed to the wethers. A sample of the yellow granules was collected and submitted for analysis. The Chemical Residues Laboratory identified the substance as lasalocid, consistent with the product label. One possible explanation for the presence of monensin was accidental purchase and feeding of the cattle mineral concentrate premix of the same brand (Olsson's Cattle Mix®), which was visually similar in its packaging.
All sheep in this mob were ear-tagged for ongoing identification. The producer observed no further losses in the following months. A total of 21/66 sheep (including many near-full-term single and twin lambs in utero) died. The producers negotiated financial compensation for the losses. CTLLS returned to the TSR to clean up the monensin granules. A bobcat was used to remove and bury the topsoil from the contaminated area and an exclusion fence was erected to restrict access to the site.
Discussion
Cases of monensin toxicity have been described in sheep, pigs, horses, dogs, cattle and poultry5. The lethal-dose 50 (LD50) of monensin is 2-3 mg/kg body weight for horses, 21.9 mg/kg for cattle, 11.9 mg/kg for sheep, 200 mg/kg for chickens, 20 mg/kg for dogs and 135 mg/kg for mice5,8. At the concentration measured in this case, only a small amount of the yellow granules would need to have been ingested to cause toxicity in sheep (~20-30g).
Clinical signs of acute monensin toxicity occur when large doses are consumed and are typically observed within 24-48 hours post-ingestion4. Affected animals are inappetent, dull and depressed, weak, ataxic, tachycardic and dyspnoeic. They will often adopt sternal recumbency and develop profuse diarrhoea prior to death5. When lower doses are consumed, the onset of clinical signs may be delayed for several days or even weeks and may include scouring, weight loss and progressive cardiac failure9. The latter is often associated with bicavitary effusion as was seen in some of the post-mortem examinations carried out during this investigation2,7.
The laboratory findings in this case reflected the myocardial degeneration and monophasic necrosis caused by excessive monensin exposure6. It is important to note that damaged cardiomyocytes do not regenerate and can only undergo repair, thus survivors of acute disease may subsequently develop myocardial fibrosis and associated cardiac insufficiency. Whilst ongoing losses were not noted in this flock in the months following the initial investigation, deaths can occur for extended periods after the exposure has stopped and will be more likely when the affected animals are exercised or stressed2.
Acknowledgements
We would like to acknowledge contributions of veterinary pathologists Dr Thomas Westermann and Dr Pedro Pinczowski (EMAI) to this case.
References
- Newsholme SJ, Howerth EW, Bastianello SS, Prozesky L and Minne JA (1983) Fatal cardiomyopathy in feedlot sheep attributed to monensin toxicosis, Journal of the South African Veterinary Association 54:29-32
- Jones A (2001) Monensin toxicosis in 2 sheep flocks Canadian Veterinary Journal 42:135-136
- Ekinci IB, Chlodowska A and Olejnik M (2023) Ionophore toxicity in animals: a review of clinical and molecular aspects International Journal of Molecular Science 24:1696
- Ferreira Silva L, de Figueiredo Gaudencio Barbosa E, de Paiva Ferreira Novaes E, Junqueira Borges JR, Mendes de Lima EM and Botelho de Castro M (2016) Clinical and pathological changes in sheep during a monensin toxicity outbreak in Brasilia, Brazil Asian Journal of Animal and Veterinary Advances 11:73-78
- Confer AW, Reavis DU and Panciera RJ (1983) Light and Electron Microscopic Changes in Cardiac and Skeletal Muscle of Sheep with Experimental Monensin Toxicosis Veterinary Pathology 20:590-602
- McGavin MD and Zachary JF (2007) Pathologic Basis of Veterinary Disease (Fourth Ed.) p1012 Mosby Elsevier
- Smith BP (2009) Large Animal Internal Medicine (Fourth Ed.) p1719 Mosby Elsevier
- Bastianello SS (1988) Ionophore toxicity in sheep Journal of the South African Veterinary Association 59(2):105
- Nation PN, Crowe SP and Harries WN (1982) Clinical Signs and Pathology of Accidental Monensin Poisoning in Sheep Canadian Veterinary Journal 23:323-326